"What We Cannot Yet Measure: Traditional Chinese Medicine and the Limits of Modern Science"
"The greatest obstacle to discovery is not ignorance — it is the illusion of knowledge." — Daniel J. Boorstin

A Response to the Pseudoscience Claim — A Practitioner’s Rebuttal
Opening Statement: This Is Not a Team Sport
Let us begin with something important: this rebuttal is not written from a place of tribal loyalty or institutional rivalry. It is not a declaration of war on Western medicine. It is, in fact, written by someone who loves Western medicine — who has been saved by it personally, who continues to study it rigorously, and whose academic training demands it.
Both my Master’s degree and my current doctoral program require thorough, examined knowledge of human anatomy and physiology, biology, pathophysiology, biochemistry, and pharmacology. I have sat with these disciplines not as an outsider looking in, but as a student committed to understanding the full landscape of human health. I hold Western medicine in genuine respect.
It is precisely because of that respect — and that depth of study — that I find the dismissal of Traditional Chinese Medicine as pseudoscience not just wrong, but scientifically incoherent. The critique does not come from a more rigorous place. It comes from a less curious one.
This is not about which tradition ‘wins.’ It is about what actually serves the patient. And on that question, the evidence — honestly reviewed — demands a far more humble and integrated answer than the pseudoscience label allows.
I. TCM Is a Complete Medical System — Not a Single Modality
Perhaps the most fundamental error in the pseudoscience critique is the conflation of Traditional Chinese Medicine with acupuncture alone. This is the equivalent of reducing Western medicine to the prescription pad. TCM is a comprehensive, integrated medical system encompassing:
• Acupuncture and moxibustion
• Chinese herbal medicine — arguably the most extensively researched domain within TCM
• Therapeutic movement: Tai Chi (Taijiquan) and Qigong
• Breathwork and meditative practice
• Dietary medicine and lifestyle medicine
• Tuina (therapeutic bodywork)
Each of these carries its own substantial body of research. Chinese herbal medicine in particular has an enormous and rapidly growing evidence base spanning oncology, reproductive medicine, dermatology, gastroenterology, psychiatry, and immunology. Dismissing all of TCM based on acupuncture trials alone — or on a single application of a single modality — is not scientific reasoning. It is category error.
II. Chinese Herbal Medicine — Evidence From the Clinics and the Literature
Reproductive Medicine and Fertility
Chinese herbal medicine has demonstrated significant and reproducible outcomes in reproductive medicine — an area where Western medicine frequently has little to offer short of expensive, physically demanding, and emotionally taxing interventional procedures.
A meta-analysis of 20 randomized controlled trials involving 1,721 women found that combining Chinese herbal medicine with IVF produced a statistically significant doubling of clinical pregnancy rates compared to IVF alone:
“Combination of CHM and IVF significantly increases clinical pregnancy rates (OR 2.04, 95% CI 1.67–2.49, p<0.00001) and ongoing pregnancy rates (OR 1.91, 95% CI 1.17–3.10, p=0.009).” — PLoS ONE, 2013
A 2025 clinical study of women with low ovarian reserve — among the most clinically challenging fertility presentations — found live birth rates of 32% in the herbal medicine group versus 5% in controls, rising to 42% when combined with IVF:
“CHM-only treatment was significantly associated with an increased likelihood of live birth (OR: 8.98, p=0.001).” — Medicina, 2025
A 2023 review confirmed that Chinese herbal medicine supports IVF outcomes through multiple documented biological mechanisms: improving ovarian function, promoting endometrial receptivity, regulating immune function, inhibiting oxidative stress, and reducing psychological distress during treatment.
Dermatology, Digestion, and Women’s Health
The herbal pharmacopeia has demonstrated efficacy in eczema, psoriasis, inflammatory bowel conditions, endometriosis, dysmenorrhea, perimenopausal symptoms, and functional gastrointestinal disorders. These are precisely the areas where conventional medicine most often offers long-term suppression rather than resolution — corticosteroids, hormonal manipulation, and symptom management without addressing underlying cause. Chinese herbal medicine works from a fundamentally different diagnostic framework, one oriented toward root pattern rather than symptom control, and the clinical outcomes reflect that difference.
III. Pain and Orthopedics — The Gap That TCM Fills
One of the clearest indictments of the pseudoscience critique is the state of Western medicine’s management of chronic musculoskeletal pain. For patients not yet meeting the threshold for surgery, conventional medicine offers anti-inflammatories, muscle relaxants, opioids, and physiotherapy — none of which address underlying pathology, and several of which carry serious, well-documented risks of harm.
Surgery, when it arrives, carries its own sobering record. Published data on lumbar spinal surgery is not encouraging:
“The lumbar spinal operation has a 10% to 46% failure risk... Success rates fall to around 30% after a second back surgery, 15% after the third, and to 5% after the fourth surgery. There may be over 80,000 failed back surgeries per year in the United States.” — American Journal of Medicine
Chronic post-surgical pain is now a formally recognized clinical entity. Between 10% and 50% of surgical patients develop persistent pain after their procedure — and research confirms this rate has not improved in decades:
“Despite significant progress in basic pain research and the increasing volume of surgeries worldwide, CPSP prevalence has remained unchanged over the past decades, raising concerns regarding the effectiveness of applied preventive strategies.” — Frontiers in Pain Research, 2023
We ask directly: by what standard is TCM held to higher evidentiary demands than surgical interventions offered as standard of care, with failure rates that would be considered unacceptable in any other domain of medicine?
TCM approaches musculoskeletal pain from a whole-systems perspective. Rather than managing symptoms until a patient qualifies for surgery, it works to resolve the underlying pattern of imbalance — treating the terrain, not just the crisis. Clinical experience, supported by a growing research literature, indicates that TCM does not merely manage chronic pain but can achieve genuine resolution in cases that conventional medicine considers permanent and unresolvable. We would welcome rigorous long-term comparative studies. We note that such studies are rarely funded by institutions with a financial stake in surgical and pharmaceutical outcomes.
IV. Mental Health, the Shen, PTSD, and the Opioid Pipeline
In TCM, the Heart is the residence of the Shen — a concept encompassing consciousness, emotional stability, mental clarity, and the capacity for genuine psychological integration. This is not poetic metaphor. It is a functional clinical framework that maps the relationship between somatic experience, autonomic regulation, and the health of the mind. Western psychiatry, in its own language, is only now beginning to formally describe the bidirectional pathways between nervous system state and psychological health that TCM has navigated clinically for over two thousand years.
Depression
A 2022 systematic review and meta-analysis of 16 randomized controlled trials found that acupuncture combined with antidepressants significantly outperformed antidepressants alone on validated depression scales, while simultaneously reducing antidepressant-related adverse effects:
“Acupuncture along with antidepressants reduced HAMD-17 scores (SMD −0.44, 95% CI −0.55 to −0.33, p<0.01).” — Journal of Integrative Medicine, 2022
A 2025 meta-analysis with trial sequential analysis confirmed that acupuncture combined with antidepressants demonstrated therapeutic advantages as early as one week post-treatment, while markedly reducing medication side effects. It is worth placing this in context: despite more than 40 antidepressant medications currently on the market, half of patients fail to achieve remission with optimized pharmaceutical treatment. This is not cited to dismiss pharmacology. It is context that makes the dismissal of TCM alternatives intellectually inconsistent.
PTSD and the Opioid Pipeline: A Created Crisis
Post-traumatic stress disorder represents one of the most treatment-resistant conditions in modern psychiatry — and one of the most consequential, particularly in veteran populations. Research into acupuncture for PTSD has expanded significantly, with results that demand serious attention:
“The first published RCT showed efficacy equivalence between acupuncture and group Cognitive Behavioral Therapy, and superiority to waitlist control, with effect retention at 3 months.” — Frontiers in Behavioral Neuroscience, 2023
“One RCT showed no statistical difference between acupuncture and selective serotonin reuptake inhibitors (SSRIs).” — Systematic Review, PMC
That acupuncture performs comparably to gold-standard PTSD treatments — without side effects, dependency risk, or the physiological burden of long-term psychiatric medication — is clinically significant in its own right. But the story does not end there. It has a second chapter that must be named directly.
The conventional treatment of PTSD — particularly in military and veteran populations — has contributed materially to one of the most devastating public health crises in modern American history: opioid addiction. Veterans with PTSD are significantly more likely to be prescribed opioids, and the consequences have been catastrophic:
“Veterans are prescribed opioid painkillers three times more often than civilians, and many go on to develop crippling addictions.” — American Addiction Centers
“A diagnosis of PTSD was strongly associated with chronic opioid use (OR = 1.22, p<0.0001)... Nearly half a million veterans abused opioids in 2020. Eighty-eight thousand met criteria for opioid use disorder.” — National Center for PTSD / SAMHSA, 2020
“Among recent Afghanistan and Iraq veterans, 63% diagnosed with substance use disorders also met criteria for PTSD.” — National Institute on Drug Abuse
It is not a coincidence that 2012 — the height of VA opioid prescribing — also saw the highest recorded rate of veteran suicide. The opioid was not a treatment for PTSD. It was a chemical suppression of suffering that created a second, compound crisis layered on top of the first.
TCM offers a genuine alternative pathway — one that addresses the underlying psychophysiological dysregulation of trauma without creating chemical dependency, without producing the physiological effects that deepen depression and suicidality, and without the prescribing cascade that turns a trauma patient into an addiction patient. This is not a theoretical advantage. It is a clinical one. And in the context of veteran care, it may be a life-or-death one.
Medication Reduction and Tapering
One of the most underreported contributions of TCM in clinical practice is its capacity to support patients in safely reducing or tapering medications that have become burdensome, dependency-forming, or no longer effective — antidepressants, anxiolytics, opioids, sleep medications. For many patients this is not a secondary benefit. It is the primary reason they seek TCM care. The clinical experience of practitioners worldwide, supported by a growing research literature, is that TCM provides the physiological and psychological scaffolding that makes medication reduction not merely possible but sustainable.
V. On Placebo — The Argument Runs Backwards
One of the most persistent claims against acupuncture is that it works because patients want it to work — that the outcome is a product of belief, expectation, and the warm attention of a practitioner. This is the placebo argument, and it sounds plausible in the abstract.
In clinical practice, it collapses immediately.
The patients who present to TCM practitioners — particularly for pain — are, in the overwhelming majority of cases, not believers. They are the opposite. They are patients who have exhausted the conventional system. They have tried the medications, the injections, the surgeries, the physiotherapy. They arrive at the TCM clinic not with hope but with resignation — skeptical, often cynical, sometimes openly dismissive of what they are about to try.
“I have no idea how sticking needles in me is going to help. But I’ve tried everything else.”
This is not an anecdote. It is the modal clinical presentation in TCM pain practice. These patients arrive as atheists. They leave often as agnostic but mostly among the converted. Not because they were primed to believe — but because something happened in their body that they did not expect and cannot explain away.
If placebo effect were the primary mechanism, we would expect the strongest outcomes in the most suggestible patients — those who came in with high hope and strong belief. The clinical reality is precisely the reverse. The most skeptical patients, those with the least expectation of benefit, frequently report the most dramatic and unexpected responses. This is not consistent with a placebo mechanism. It is consistent with a real physiological effect acting independently of belief.
The placebo argument also fails to account for the reproducible efficacy of TCM — including acupuncture and herbal medicine — in pediatric and animal populations, where the expectation effect is negligible or absent entirely. You cannot convince an infant or a horse that they feel better.
The Veterinary Evidence: A Case Study in Non-Placebo Efficacy
Veterinary acupuncture deserves particular attention in this discussion, because it represents perhaps the cleanest natural experiment available to resolve the placebo question. Animals have no understanding of the therapeutic context, no cultural conditioning about needles, no relationship dynamic with a practitioner that could generate expectation effects, and no capacity to report improvement in order to please a clinician. If acupuncture works in animals, it works on physiological grounds alone.
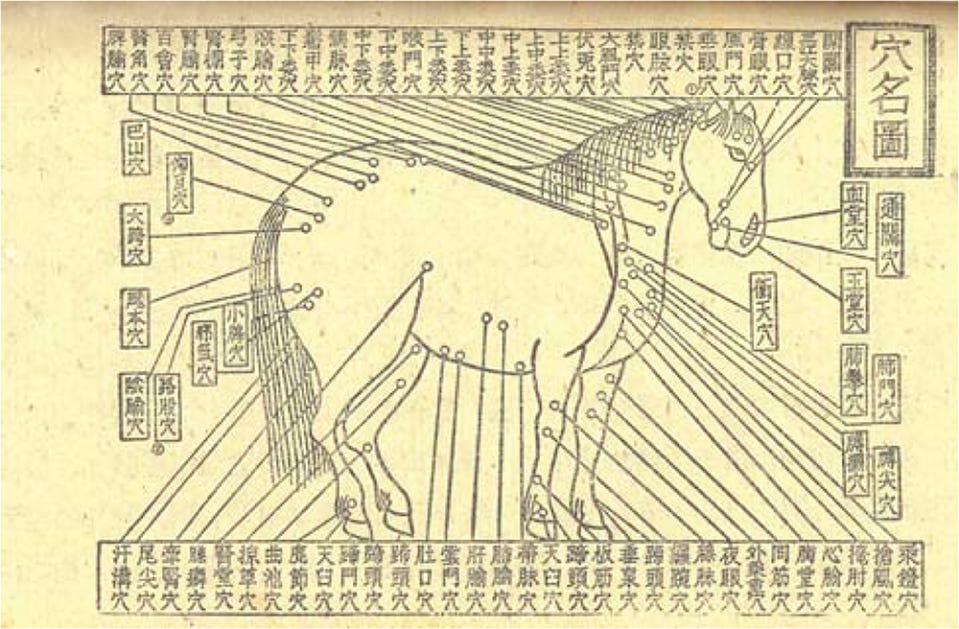
The history of veterinary acupuncture is ancient and well-documented. Chinese “horse priests” — dedicated caretakers of military horses — practiced acupuncture during the Shang and Zhou Dynasties as far back as 2000–3000 BCE. The earliest surviving veterinary acupuncture textbook, Bo Le Zhen Jing (Bole’s Canon of Veterinary Acupuncture), dates to approximately 659–621 BCE — predating the founding of the first Western veterinary college by more than 2,300 years. During the Zhou Dynasty, veterinary acupuncture was formally designated as a separate branch of traditional Chinese medicine. The ancient Chinese mapped 173 acupuncture points in animals, a system that has been continuously refined and applied across millennia.
In the United States, veterinary acupuncture was formally introduced in 1971. The International Veterinary Acupuncture Society (IVAS) was founded in 1974 and held its first certification examination in 1975 with 80 members. Today the field has grown substantially: according to the American Board of Veterinary Acupuncture’s 2024 petition to the American Veterinary Medical Association, between 4,000 and 5,000 licensed veterinarians in the United States have now completed acupuncture certification through one of six accredited training organizations. Approximately 80% work primarily with small animals, 10–20% with equine patients, and the remainder with farm animals, exotics, and zoo species.
Veterinary acupuncture is not fringe practice. It is taught at university veterinary programs, integrated into specialty and rehabilitation clinics, and is now actively seeking formal specialty recognition from the AVMA — a process that requires demonstrating a scientifically grounded and distinct scope of practice. The AVMA itself has admitted the American Academy of Veterinary Acupuncture (AAVA) as a constituent allied organization.
The research underpinning veterinary acupuncture mirrors its human counterpart in many key areas. Studies have documented analgesic effects mediated by the release of beta-endorphins, serotonin, and other neurotransmitters at acupuncture points — the same neurochemical mechanisms observed in human studies. Acupuncture points in animals have been found to correspond to areas of high density of free nerve endings, mast cells, arterioles, and lymphatic vessels, providing an anatomical basis for their effects. Clinical applications include chronic pain, musculoskeletal conditions, neurological rehabilitation, gastrointestinal disorders, and reproductive medicine.
Crucially, much of the foundational NIH acupuncture research that led to the landmark 1997 consensus statement on acupuncture efficacy was conducted using animal models. The animals in those studies were not experiencing placebo. They were demonstrating measurable physiological responses — changes in neurotransmitter levels, inflammatory markers, and pain thresholds — that formed the evidentiary basis for the NIH’s conclusions about human clinical applications.
In short: the veterinary record does not merely support the placebo rebuttal. It constitutes an independent, parallel body of evidence for the physiological reality of acupuncture — evidence gathered from patients who had absolutely no idea they were being treated.
VI. The Sham Acupuncture Problem — A Methodological Critique
The most frequently cited evidence against acupuncture is that sham acupuncture — needling at incorrect points, or using retractable placebo needles — performs similarly to verum acupuncture. This finding is presented as proof of placebo. It is, in fact, evidence of a methodological problem.
Within classical TCM, the body’s energetic architecture functions as a unified, continuous field. The meridian network is not a collection of isolated points but an interconnected circulatory system of Qi. Introducing a needle anywhere into the living system produces a systemic response. The analogy is instructive: dropping a stone anywhere in a pond creates a wave across the entire surface. The difference between random needling and skilled, diagnostically-informed acupuncture is not the presence or absence of effect — it is the precision, intentionality, and clinical sophistication of the intervention. The difference between dropping a stone in water and harnessing that same water to generate hydroelectricity.
Designing a sham control that inadvertently delivers a real physiological intervention, then concluding that the intervention produces no specific effect, is a failure of experimental design — not evidence of inefficacy. This point has been raised by acupuncture researchers, biostatisticians, and integrative medicine academics for over a decade. It has not been adequately answered by those who continue to cite sham trial data as definitive.
VII. The Evidence Exists — The Measurement Tools Are Insufficient
TCM has a substantial and legitimate evidence base. Acupuncture for chronic pain has been evaluated in some of the most rigorous meta-analyses in complementary medicine, consistently demonstrating statistical superiority to controls. Chinese herbal medicine, Tai Chi, and Qigong research spans thousands of peer-reviewed publications across oncology, cardiology, neurology, geriatrics, and psychiatry. The Cochrane Collaboration, JAMA, The Lancet, and the British Medical Journal have all published favorable findings.
The problem is not that evidence does not exist. The problem is that the dominant tools for measuring medical efficacy — designed for single-molecule, single-target, single-outcome pharmaceutical trials — are poorly matched to the nature of a whole-systems medicine.
TCM diagnosis is individualized: two patients presenting with the same biomedical diagnosis will frequently receive entirely different treatments based on their constitutional pattern, pulse, tongue presentation, and symptom constellation. Randomized controlled trials that assign a uniform protocol to all patients with a given diagnosis are, by design, testing something other than TCM as it is actually practiced. This is not a defense of low-quality evidence. It is a call for research methodologies sophisticated enough to evaluate what is actually being investigated.
VIII. 2,600 Years Is Not an Accident
This medicine has been practiced, systematized, refined, challenged, and transmitted across more than two and a half millennia. It has endured the rise and fall of dynasties, epidemics, colonial suppression, and in the modern era, sustained institutional skepticism from Western medicine. Generation after generation of practitioners and patients — across radically different cultures, geographies, and historical circumstances — have continued to use and refine it because it produced results.
Medical practices that are demonstrably false do not survive this way. They are abandoned. The persistence of TCM is not cultural inertia. It is the longest-running clinical evidence base in human history.
It is also worth noting the behavior of the conventional medical establishment itself. Physicians, chiropractors, nurses, and physical therapists across the Western world are now seeking acupuncture training. The US Department of Veterans Affairs, the US military, and major academic medical centers including the Mayo Clinic and Cleveland Clinic have integrated acupuncture into standard care protocols. Insurance coverage is expanding. These are evidence-responsive institutions. Their adoption of TCM modalities is not sentiment. It is a clinical signal.
IX. A Question of Intellectual Consistency
We ask, finally, for intellectual consistency in the application of evidentiary standards.
A significant number of pharmaceutical interventions prescribed daily were approved on evidence no stronger — and in several cases considerably weaker — than what TCM research routinely produces. Multiple drug classes proven to perform at or below placebo in independent replication remain in widespread clinical use. The opioid epidemic, one of the most catastrophic pharmaceutical failures in modern history, was built on a foundation of clinical trials, regulatory approval, and professional endorsement. We cite this not to dismiss biomedicine, but because critics of TCM have not applied equivalent scrutiny to the system they implicitly defend.
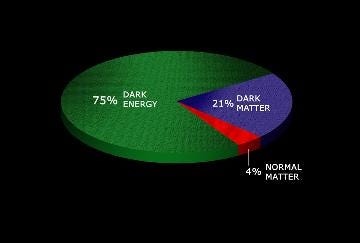
Modern physics has established that the universe contains forces, fields, and phenomena — dark matter, quantum fields, the behavior of subatomic particles — that are real, reproducibly measurable in their effects, yet not classically explicable. Science accepts these realities because the evidence of their effects is consistent. We ask for the same framework to be applied to a system of medicine whose effects have also been consistent — across populations, practitioners, centuries, and cultures.
The question is not whether TCM works. The question is whether our current instruments are sophisticated enough to fully explain why. Dismissing what we cannot yet measure is not science. It is the premature closure of inquiry — the very antithesis of what science claims to stand for.
Closing
TCM is not asking to be exempt from scrutiny. It is asking to be scrutinized fairly — with the same intellectual rigor, the same methodological creativity, and the same willingness to follow evidence that we rightly demand of any healing tradition.
This rebuttal is written not in opposition to Western medicine but alongside it — by a practitioner who has studied both, respects both, and believes deeply that the patient is best served when the full spectrum of human healing knowledge is brought to bear. The question was never which medicine is right. The question is always: what does this patient need?
We are confident that when TCM is scrutinized honestly, without institutional bias or premature conclusion, the medicine will speak for itself.
It has been doing so for 2,600 years.
Barry Danielian is a licensed acupuncturist (L.Ac.) and a board-certified herbalist. Currently a doctoral candidate at Daoist Traditions College of Chinese Medical Arts, where he studies within the Jade Purity lineage of renowned Master Jeffrey Yuen. He has, for 40 years been one of the most in-demand trumpet players in NYC, and a longtime member of the E Street Horns. He writes at the intersection of classical Chinese medicine, martial arts, music, and spirituality. Bridging ancient wisdom with modern life.
Selected References
Ried K, et al. Can Chinese Herbal Medicine improve outcomes of in vitro fertilization? PLoS ONE. 2013; doi:10.1371/journal.pone.0081650
Wu MH, et al. Effect of Chinese Herbal Medicine on Pregnancy Outcomes in IVF Patients with Low Ovarian Reserve. Medicina. 2025; doi:10.3390/medicina61091571
Chen Y, et al. Chinese herbal medicines as complementary therapy to IVF-ET. Journal of Assisted Reproduction and Genetics. 2023; doi:10.1080/14647273.2023.2266619
Tang X, et al. Efficacy and underlying mechanisms of acupuncture therapy for PTSD. Frontiers in Behavioral Neuroscience. 2023; doi:10.3389/fnbeh.2023.1163718
Hollifield M, et al. Acupuncture for PTSD: A Systematic Review. Journal of Nervous and Mental Disease. 2007.
Xu S, et al. Can acupuncture enhance therapeutic effectiveness of antidepressants? Journal of Integrative Medicine. 2022; doi:10.1016/j.joim.2022.01.008
Smith CA, et al. Acupuncture for Depression: A Systematic Review and Meta-Analysis. PMC. 2019; PMC6722678
He L, et al. Acupuncture combined with antidepressants for mild-to-moderate depressive disorders. PMC. 2025; PMC12741110
Chan PW, Peng P. Failed Back Surgery Syndrome. Pain Medicine. 2011; doi:10.1111/j.1526-4637.2011.01089.x
Alshammari SA, et al. Prevalence of Chronic Pain After Spinal Surgery. Cureus. 2023; doi:10.7759/cureus.41841
Guerrero Moreno JM, et al. Chronic postsurgical pain and transitional pain services. PMC. 2025; PMC11877094
Bernardy N, Montano M. Opioid Use Among Individuals with PTSD. National Center for PTSD, VA. 2019.
SAMHSA. Results from the 2020 National Survey on Drug Use and Health. 2020.
National Institute on Drug Abuse. Substance Use and Military Life. NIDA DrugFacts. 2025.
Xie H, Eckermann-Ross C. Veterinary Acupuncture. Veterinary Clinics of North America: Exotic Animal Practice. 2012.
Koh RB, Harrison TM. Veterinary Acupuncture: From Evidence to Clinical Application. Veterinary Clinics of North America: Exotic Animal Practice. 2023.
American Board of Veterinary Acupuncture (ABVA). Letter of Intent for Specialty Recognition. American Veterinary Medical Association. 2024.
Acufinder.com. History of Veterinary Acupuncture. Citing Shang/Zhou dynasty horse priest traditions, 2000–3000 BCE.
NIH Consensus Statement on Acupuncture. National Institutes of Health. 1997.
Speaking for myself, I can share that my health & wellness experience has been forever changed for the best after being treated with Chinese herbal medicine! No only did it strengthen my immune system but has healed me tremendously from anxieties & inflammation, I am always seeking to grow in my knowledge of how my continued use can elevate my health to its highest capabilities! I will be reaching Dr. Danielian for services. Thank you for your incredible breakdown and adding your knowledge to this well written article.